
In this article I will look into the history and developments of forward surgical care that resulted in the attachments of a platoon (or Hospitalization Unit (HU) of a Field Hospital to the 4th AD. It is a closer look at one of the aspects discussed in the article Fixing the weakest link in the chain. I think it is important to start with some definitions, especially as the term “field hospital” is often used to describe all types of military hospitals. The Oxford English dictionary’s definition is: “a temporary or mobile military hospital; esp. one set up near a combat zone to treat the wounded”. Merriam-Webster’s definition is: “a military organization of medical personnel with equipment for establishing a temporary hospital in the field”. It this article the term describes a specific type of military hospital within the US Army of WW2 with its own TO&E and purpose, called Field Hospital, as there are General Hospitals, Evacuation Hospitals and Station Hospitals.
To understand the role that the platoons of the field hospitals played during WW2 in the US Army, we must first look at the history of forward surgical care since WW1
In many respects WW1 turned out the be a war that the armies of the combatant nations were not prepared for. From a medical point of view the destructive power and range of modern weapons and the long durations of battles proved that the organization of evacuation and treatment that the armies entered the war with was inadequate. The long range of artillery resulted in hospitals being kept far away from the front. This in turn meant long evacuation distance and time for the wounded, with detrimental effects on the health of the wounded soldiers. From 1915 the armies started to experiment with ways of moving surgical care for the most severely wounded forward, closer to the front. Moving surgical care forward not only meant sending surgical teams forward, but also hospital beds for post-operative care. The British Army’s solution was to add surgical care to its Casualty Clearing Stations (CCS). The French Army created Ambulance Chirugical Automobile (ACA) units. When the US entered WW1, it essentially copied the French method but called it Mobile Hospitals (MH). The MHs were tasked with resuscitative surgical care of the non-transportable casualties, aimed at making these casualties transportable, ready to be evacuated to the rear. Definitive surgical care would be performed in the evacuation hospitals. The MHs were intended to be distributed as one per division, operating directly next to the other division hospitals.
When the war finally returned to mobile warfare in 1918 the best solution for forward surgical care was complicated by another need besides surgical and post-operative capability: mobility. The MHs proved to be transportable rather than mobile as their TO&E lacked the needed transportation capacity to transport the entire hospital.
Between WW1 and WW2, the US Army Medical Department evaluated the lessons of WW1. Discussions began about the Mobile Hospitals. Was forward surgical care still needed? Did the use of the newly developed blood plasma and sulfa drugs not buy enough time to evacuate the wounded to the evacuation hospitals? And if forward surgical care was still needed, did each division still need its own unit, now that the old division structure with four regiments (around 12,000 infantrymen) was reduced to three regiments (around 7,000 infantrymen). The estimation was that only a small percentage of the casualties needed this forward surgical care. Surely smaller divisions also meant fewer non-transportable casualties per division. And if forward surgical care was still needed, what was the best compromise between surgical care, post-operative care and the need for mobility?
In the end the US Army Medical Department decided to keep its forward surgical care capability but move it from the division to the Corps area with 4 newly created hospital units per field army. The newly created hospital unit was called Surgical Hospital (SH). It consisted of one surgical unit and two hospitalization units of 200 beds each (the first TO&E for an SH showed a bed capacity of 250 beds in total, so during its development the units became much bigger). The thought was that these hospitalization units could be deployed laterally from each other, for instance during times when the front was static. They could also be deployed “vertically” from each other and leapfrog. This way, when one hospitalization unit was receiving and treating patients (and therefore became temporally immobile), the other unit could leapfrog closer to the front. The surgical unit had 4 operating rooms and could, when reinforced with extra surgical teams, handle around 80 operations in 24 hours.
On paper this seemed like a solid plan. However, during the North African campaign, many of these ideas didn’t work out as expected. First of all, the use of blood plasma and sulfa drugs proofed to be inadequate at buying enough time for the severely wounded to be evacuated to the Corps area. Forward surgical care still needed to be given closer to the front. Also, the SH set up wasn’t working. Its hospitalization units were too large and therefore not mobile enough. During this campaign, the SHs were also not used exclusively for their intended use: they received many medical cases rather than the non-transportable surgical cases. So, the triage determining who needed the forward surgical care provided at the SH was ineffective. This was partly due to the inadequate number of hospitals in the North-African Theater at the time. The US Army Medical Department needed to reorganize using these lessons. Forward surgical care needed to be moved forward to the division area, preferably next to the division clearing stations that could do the proper triage and only send non-transportable surgical cases to the new units designated for this purpose. The new units needed to be smaller and therefore more mobile to keep up with advancing divisions. When these new units needed to move while still treating patients, other units had to take these patients over as holding units.
It is a testament to the incredible flexibility and organizational skills of the US Army Medical Department that these conclusion could be turned into concrete policies almost immediately. It simply had to add one more possible role to another type of unit that it already had designed: the field hospital.
Field hospitals were originally designed as a unit that could be deployed under several different circumstances and function accordingly. They were created to function as Station Hospitals in newly created military bases overseas. Many of these bases were too small to need a full Station Hospital.
They could also be used as temporary Evacuation Hospitals when needed. According to FM 101-10- (12 October 1944) the Field Hospitals were to be “used to cover air bases, island garrisons or sectors of ComZ when fixed bed facilities are not present and construction not feasible. Should be considered mobile type of Station Hospital. Of great value under jungle conditions where it may serve at a landing field as a small Evacuation Hospital”. As a whole unit, Field Hospital units had a capacity of 400 beds, but they were designed and trained to split into three identical units (“platoons” or “hospitalization units”). When a single platoon was deployed, it had a capacity of 100 beds, more than enough for small military bases on, for instance, islands in the Pacific. Each platoon had seven 2.5-ton trucks to ensure its mobility.
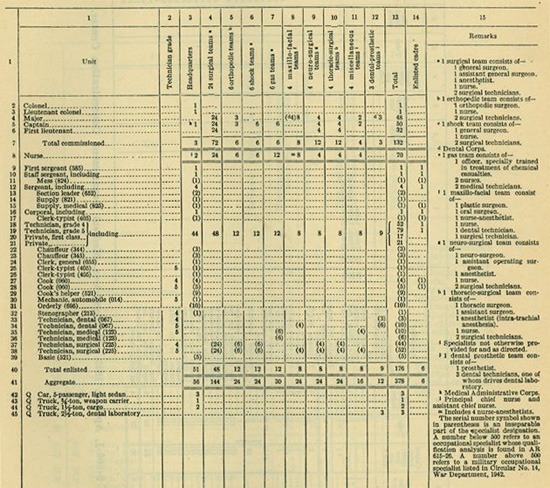
These characteristics of the field hospital platoons: a “small” 100 bed capacity and transportation capacity, made them a good solution to the need for post-operative care after forward surgical treatment. The surgical care itself could be attached to these units from the Auxiliary Surgical Group (ASG) that each field army had. These groups were essentially the “flex pool” of surgical care within the field army. Each groups consisted of 24 surgical teams, 6 orthopedic teams, 6 shock teams, 6 gas teams, 4 maxillo-facial teams, 4 neurosurgical teams and 4 thoracic surgical teams. These teams could be temporarily attached to hospitals when it was expected that extra surgical teams were needed. The field armies also had a variety of other medical units that could be deployed as temporary holding units (independent clearing or collecting companies for example). Using these three units together gave the US Army Medical Department all it needed to ensure forward surgical care in the division areas: surgical teams of the ASG for the surgical care, a platoon of a field hospital for the post-operative care, with enough transport capability to ensure the needed mobility, and finally other medical units for holding capability when the units needed to advance.
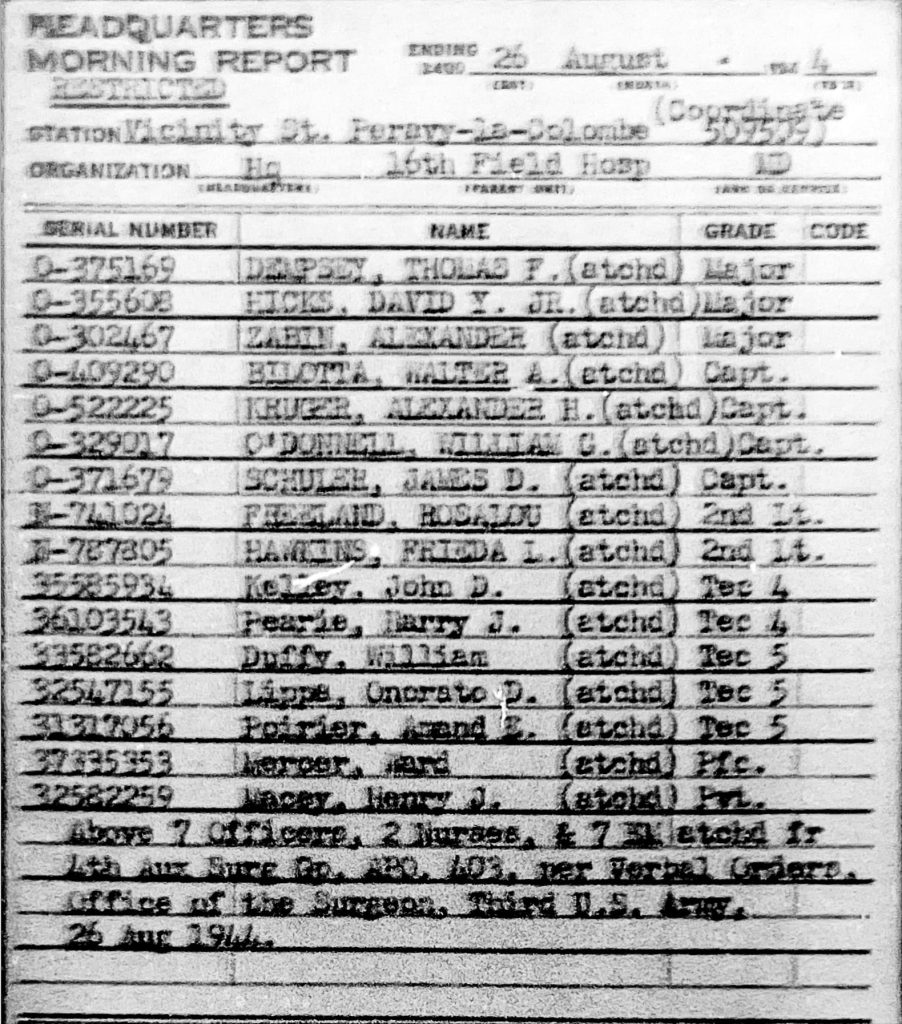
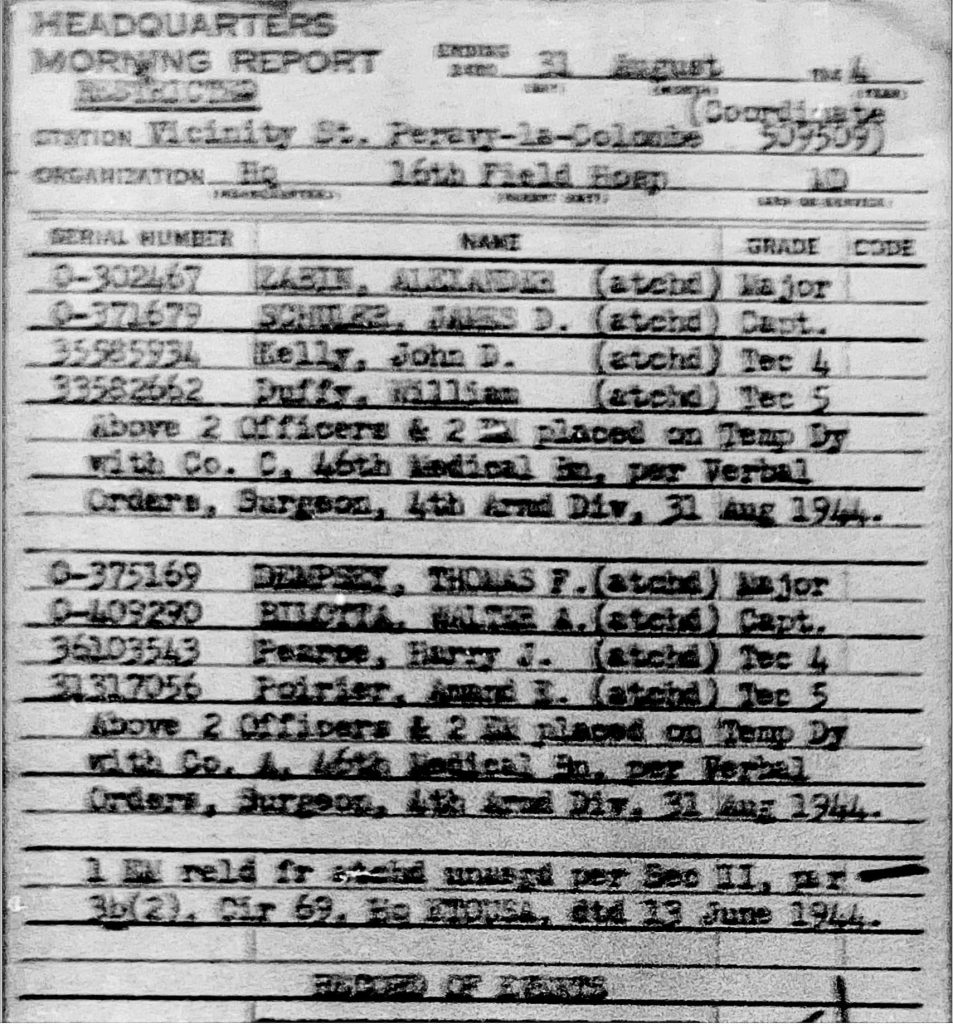
From the morning reports of the 16th Field Hospital, we can see all the relevant factors in play:
1)the hospitalization unit moving with the 4th AD(Photo history)

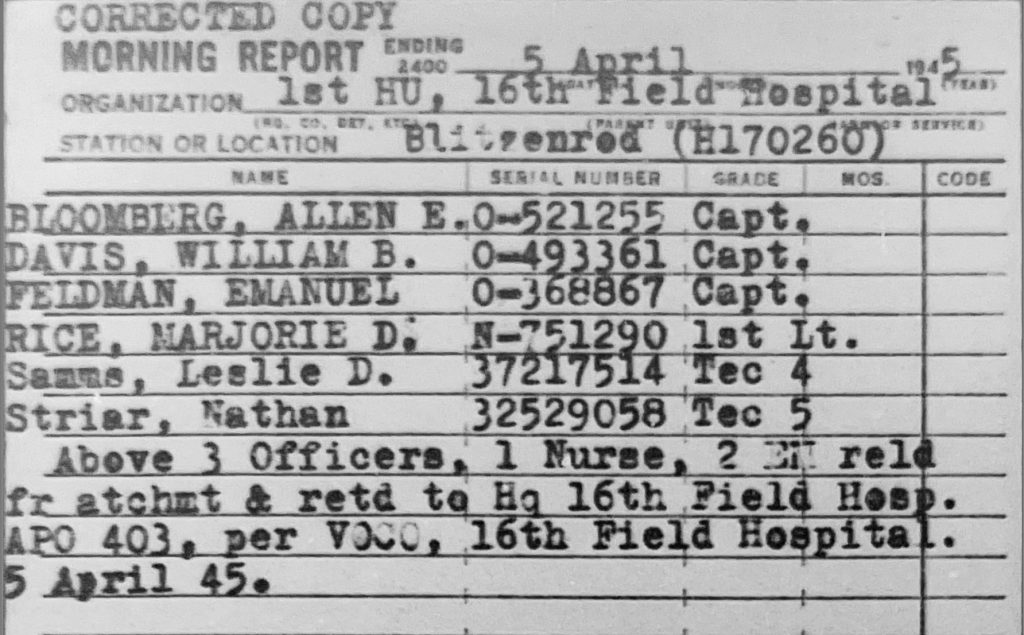
2) Surgical teams attached from 4th ASG, first to 16th FH, then to 1st platoon
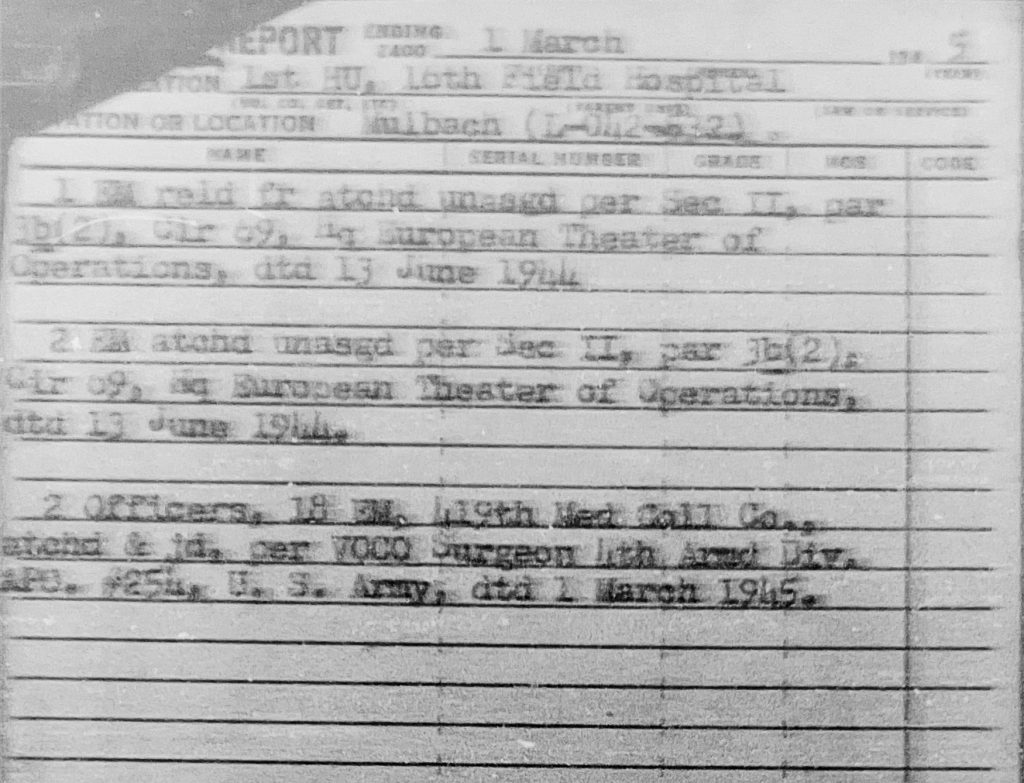
3)Units moving in as holding units. In this case 2 officers and 18 EM from the 419th Medical Collecting Company. Note that this movement of the “holding unit” was done under orders from the Division Surgeon of the 4th AD (VOCO Surgeon 4th AD), showing that the 1st platoon, 16th FH’s operations were at least in close cooperation if not under direct control of 4th AD.
From the TO&E of an ASG, when can start to work out what type of surgical teams were attached to first platoon, 16th FH.
Here we see three officers Medical Corps (MC), one nurse and two technicians, making this a general surgical team.
Now, let’s look at the situation of the 4th AD. A platoon of the 53rd Field Hospital was attached to the division on August 8th, 1944. The division was located around Vannes en Lorient on the southern coast of Brittany on that date. Why it took until this date to attach a field hospital platoon to the division is unclear. Possible factors were that Third Army was activated on August 1st, 1944, during an extremely rapid advance of its VIII-Corps (which included the 4th AD). Only a few days before the distance to the established hospitals in Normandy was short enough for rapid evacuation, even for the severely wounded. But in the days that it took 4th AD to race to Lorient, the evacuation distance between its clearing stations and the nearest hospital had grown to over 100 miles, through areas that had not been completely cleared of German units. For a few days the division medical units had to improvise to care for their severely wounded casualties. The attachment of the platoon of the 53rd Field Hospital came as a big relieve.


On August 27th, 1944, the platoon of the 53rd Field Hospital was relieved from its attachment to the 4th AD, and the first platoon of the 16th Field Hospital was ordered to take its place. To help move the unit, the 4thAD send 12 additional truck, showing that the organic transportation capacity was still not enough under all circumstances.

The first platoon, 16th Field Hospital would be kept at the clearing station of the reserve medical company, attached to Division Trains .
From August 27th, 1944, for the rest of the campaign in Europe and during the early period of occupation of Germany, the first platoon, 16th FH remained attached to the 4th AD. This does not mean that all non-transportable casualties of the 4th AD were only treated at the first platoon, 16th FH. Especially during the Lorraine Campaign, during the fall of 1944, the field hospital platoons attached to the divisions of XII Corps (to which the 4th Ad was attached at the time) leapfrogged behind the front and served multiple divisions when they were set up closest to the front. This was partly because the front did not advance much during this period, but also because of a lack of suitable locations for these units during this period. A platoon of a FH could only move closer to the front after the front had moved enough and a suitable location had been found.
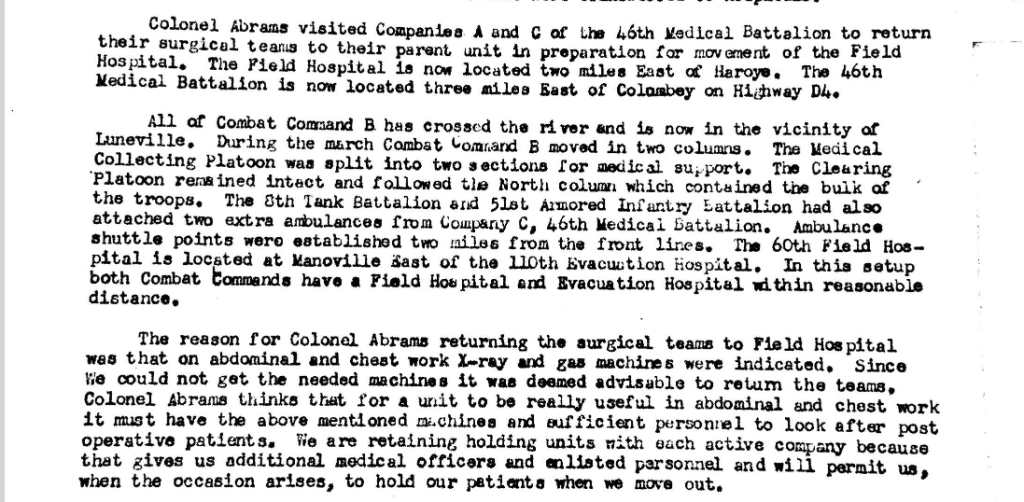
It is very interesting to note that the Division Surgeon of the 4th AD, Lt.Col. Morris Abrams, experimented with another set up in an effort to move the forward surgical care even closer to the front by organizing the same factors (surgical care and hospitalization) at the clearing stations of the division’s two combat commands. He suggested creating such a set up on August 20th, 1944, to the XII Corps Surgeon.

Starting August 30th, 1944, he attached one surgical team of the 4th ASG (attached to first platoon, 16th FH at the time) to each of the combat commands, together with sections of a Medical Clearing Company (from Third Army). This created, in effect, two “mini field hospitals”, small units that could provide forward surgical care, with a capacity of 15-20 beds each. Note that the nurses of these surgical teams were not brought forward to these “mini field hospitals” at the combat commands.

This experiment ended two weeks later, when it was found that for proper abdominal surgery an X-ray machines and a proper anesthesia apparatus (“gas machines”) were needed. Both of these items were not in the TO&E of the Medical Clearing Company.
Another event that is worth discussing is the capture of the first platoon, 16th FH on April 1st, 1945, by units of the 6th SS Mountain Division,”Nord”. On this day, the first platoon, 16th FH departed its previous location at Dieburg, Germany around 0700h. The convoy crossed the Main River and travelled north. Accompanying this convoy were the commanding officer and chief of surgery of the 106th Evacuation Hospital. They were on a reconnaissance trip to look for a suitable new location for their hospital. According to the morning report and the medical after action report of Third Army, the convoy was ambushed and captured around 0900h in the vicinity of Altenstadt, Germany, (other accounts state that these events took place further West, near Assenheim, Germany).
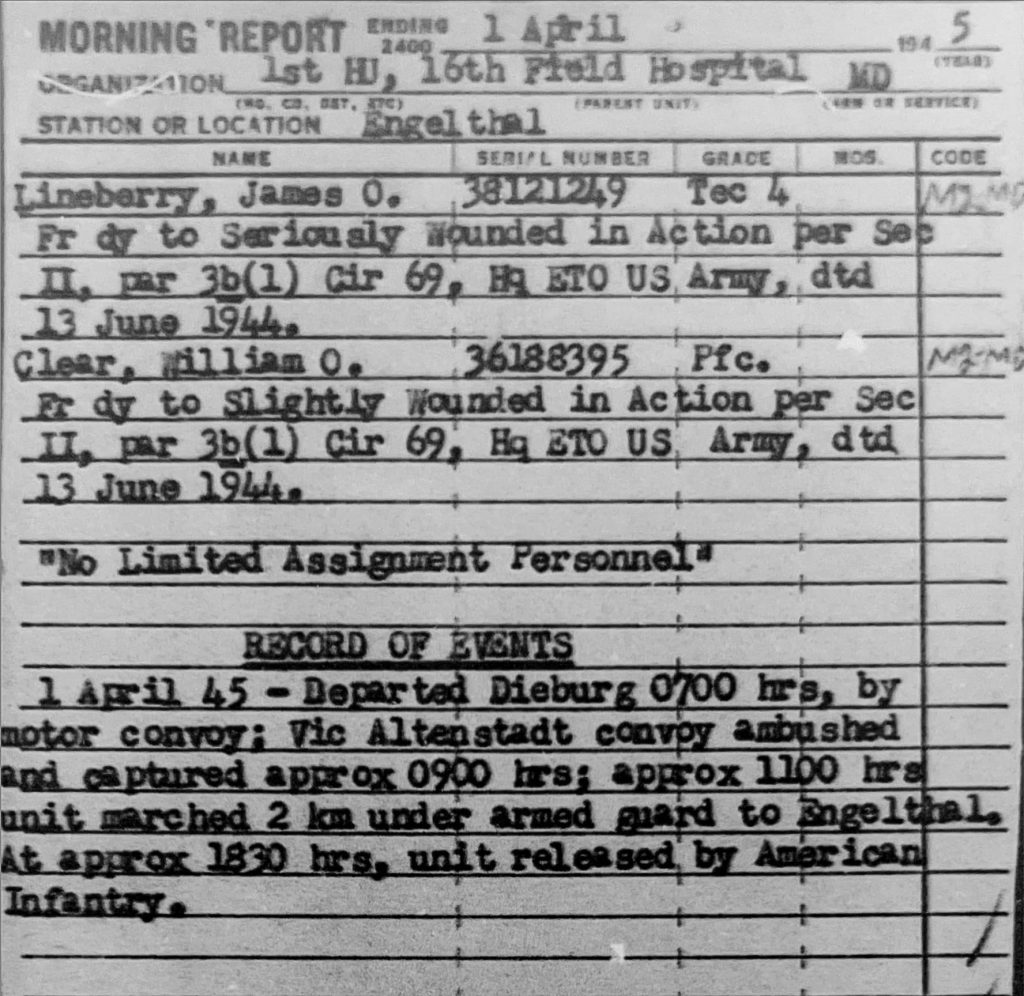

All personnel, including the nurses, were taken prisoner and were then marched 2km West to the abbey Engelthal. Unfortunately, the chief of surgery of the 106th Evac (Major Fonde) was killed in this action. After the first platoon, 16th FH was brought to the abbey Engelthal, it set up operations there and started treating wounded soldiers.

According to the memoir of General Patton: “War as I knew it”, reports of the capture of the hospital unit were accompanied by rumors of atrocities: murder and rape of hospital personnel. These rumors were later proved to be false. Personnel travelling with the hospital did report the SS troops killing German soldiers who had previously surrendered to the American troops.
According to the morning report, first platoon, 16th FH was recaptured the same day around 1830h. Other reports, such as the medical after action report of Third Army, state that the recapture of the unit took place on April 2nd, 1945. The book: Fourth Armored Division from the beach to Bavaria stated that it took even one day longer. This discrepancy is probably attributable to the fact that different groups of American prisoners were recaptured at different times by elements of the 5th and 71st Infantry Divisions.
I have not been able to determine how many casualties were treated by the first platoon, 16th FH. I did find the statistics for the entire 4th ASG, serving Third Army:
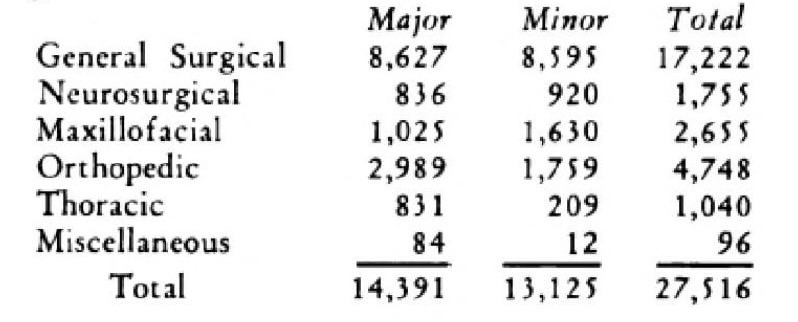
These Admission and Disposition forms help us by giving us an impression of the numbers and types of casualties that the first platoon, 16th FH treated. They also give us an impression of the number of casualties whose wounds were so severe that even the forward surgical care provided was unable to save (“DOW” Died of Wounds).


In 1945 the US Army convened General Boards to evaluate the experiences during the campaign in Northwest Europe and formulate the lessons learned. The General Board on “ the organization and equipment of medical units in the European Theater of Operations” mentions the lessons concerning the use of Field Hospitals. Its conclusions were that: “Early combat experiences in the Norh African Theater indicated the need for a mobile surgical hospital to care for severely wounded, non-transportable casualties in the vicinity of division clearing stations….. The field hospital is not entirely suited for this mission but minor modifications in the hospital and by the attachment of auxiliary surgical teams they were able to perform this function in an excellent manner”.
However, using the lessons learned, the US Army started to look for a new type of mobile surgical hospital. In the same report the General Board concludes: “It is universally agreed that there is a definite requirement for a mobile surgical hospital of fifty to seventy-five bed capacity to take care of first priority surgical casualties in the vicinity of the division clearing station”.
It also specified other characteristics needed in such a new type of hospital: “The surgical hospital unit which is to operate in the vicinity of the division clearing station must be mobile. It is essential that its mobility be derived from its own organic transportation…..A false sense of economy in transportation is obtained when the hospital unit is not completely mobile”. Another characteristic for such a new hospital unit is: “Experience has shown that there is a definite requirement for holding facilities in the first priority surgical hospital. It would be ideal to have sufficient hospitalization units to permit the hospitalization unit in its entirety to remain in place as a holding unit while another hospitalization unit is displaced forward in close support of the division.” It is interesting to note that what is suggested here is that all required functions: surgical care, post-operative care and mobility are combined in the new hospital unit rather than meeting these requirements by using different teams and units. It is also interesting to see that the bed capacity that is needed is reduced to 50 to 75 beds.
In the end all these lessons resulted in the formation of a new mobile surgical hospital known as a MASH (Mobile Army Surgical Hospital) in August 1945. It had a bed capacity of 60 beds, assigned rather than attached surgical teams and 10 2.5-ton trucks with trailers to ensure its own mobility.
The last MASH unit disappeared in October 2006, when it was converted to a Combat Support Hospital. This is the organizational successor of the MASH, continuing the lineage of military hospital units providing forward surgical care since WW1.